Barriers to averting dose
Barriers to averting dose
The principal barriers to averting dose are likely to be:
- The failure to agree and attempt to promulgate appropriate advice;
- The failure to reach the affected people to warn them and then give them accurate detailed information and appropriate advice in a form that they understand and can achieve;
- The decision of the recipients not to act on the advice; or
- The inability of the recipients to follow the advice (i.e., find a solid building in which to shelter).
Formulating advice
The main concern relating to a radiation emergency, as opposed to other emergencies, is the uncontrolled release of radioactive material potentially leading to additional radiation doses to members of the public and contamination of the environment. We attempt to reduce these additional radiation doses because at large doses radiation can cause illness and death and, at low doses, it is assumed to increase the chances of cancer in the longer term.
For atmospheric releases, the urgent aspiration is usually to reduce inhalation doses as the plume passes by and the medium-term aspiration is to reduce ingestion doses resulting from the consumption of contaminated food. Other dose routes, such as cloud shine during the event and ground shine after the event are also taken into consideration but tend to result in lower doses in the urgent phase. Environmental contamination is the long-term issue. Following the Fukushima accident the ground gamma dose rates became an important and contentious subject of debate, particularly the dose rate in school playgrounds.
Great efforts have been made to quantify the “costs” related to exposure to low levels of radioactivity (a few to a few hundred mSv) and to compare these to the costs, in terms of direct expense, inconvenience and risk, associated with protective actions. In the UK, PHE have published advice in the form of Emergency Reference Levels (ERLs) stating that the balance point for shelter is between 3 and 30 mSv, evacuation between 30 and 300 mSv (whole body doses and the taking of stable iodine between 30 mSv and 100 mSv (iodine dose to the thyroid). These values are for averted dose.
It is worth noting that the term “evacuation” describes the act of moving people and maybe animals from a dangerous place to somewhere safe. It is implicitly assumed that these people will be allowed back to their homes when the danger has passed. Clearly the ability and confidence to return home soon after the event has an important effect on the long-term impacts of the event. Relocation, where the person is required to move home after the event, may prove to be stressful in the long-term but so to might be living in a contaminated area despite official assurances that the risks related to that contamination are low.
From the purely technical point of view, an emergency response and the public communications within it, would be considered to be a success if public radiation doses were kept below 100 mSv for the most exposed individuals and if protective actions were enacted where they averted more than the relevant lower ERL and not too many people were inconvenienced, let alone hurt, by protective actions that did not reduce their dose by sufficiently worthwhile levels (either their actual projected dose was too low or the protective action failed to avert dose as intended).
The rather naïve view has been that if the authorities provide prior information to the public based on this dry scientific analysis, the public will then make better provision for emergency response. If the authorities then provide information and advice during the emergency about the minimal impact of low radiation doses and the appropriate levels of protective actions the public will make better decisions during and after the emergency. This will reduce their additional radiation dose and therefore reduce the consequences of the nuclear or radiological emergency. As a result of this, the people who took protective actions and those exposed to low levels of radiation dose but did not take protective actions, and those who think that they might have been exposed to very low levels, are all reassured and return to life as normal.
This assumes a high level of scientific literacy, a confidence in the science and the reporting of the dose implications of the event (which requires clarity and consistency of message), and a trust in the expertise and trustworthiness of the industry, local authority and government spokespersons. At a push, just the trust in the talking heads might be enough.
A more nuanced set of targets for an off-site plan might include the desire to reassure members of the public and provide the support they require to stay safe and comfortable if asked to stay indoors for any length of time, if asked to take tablets or evacuate their homes and offices and, particularly if they require, or believe they might require, radiation monitoring and decontamination.
A potential problem with protective action zones.
Any protective action zone will obviously have a line between those advised to take protective actions and those not. You can expect issues related to this such as
the covid-related BBC News headline “Leicester lockdown: Boundary line branded 'stupid' by residents” where people subject to a local lockdown could see open pubs across the
road (BBC, 1/7/20).
This zone was designed on a post-code basis.
How do you explain to one person that they should take protective actions while explaining to a near neighbour that they have nothing to worry about?
Leicestershire County Council said the boundary had been drawn up rapidly and was "an imprecise science". Maybe not the best choice of words while being absolutely accurate – taking more time and having perfect data would not solve the presentational difficulty.
It was also reported that the shadow health secretary and Leicester South MP Jonathan Ashworth said people in the city were confused by the rules. (So don’t expect uncritical support from local elected members).
A recent FEMA report (FEMA, 2021 - Key Planning Factors and Considerations
For Response to and Recovery from a Chemical
Incident discussing preparing for chemical accidents, stresses the
importance of agreeing how decisions will be made suggesting a process whereby stakeholders agree which decisions will need to be made, the minimum information needed to
make them and the potential sources for that information. I’m not sure that the nuclear industry has achieved this level of detail in the
decision-making process which is a weakness.
 FEMA Action item
FEMA Action item
Making decisions about protective actions in a nuclear or radiological emergency is going to be difficult. The technical task requires determining the projected and avertable dose as a function of location and time around the area surrounding the site. This requires the integration of information about the accident’s starting conditions, the magnitude of any release and its physical and chemical properties and how they may vary in the future, the weather, particularly the wind speed and direction, how any released radioactivity will disperse and the location and likely activities of alerted and non-alerted members of the public. Any decisions will have political implications (and probably input) and resource implications. However, the default protective actions that have been agreed in advance are designed to be likely to err on the side of over-reaction.
Reaching the target audience, Communications channels
It is also important to consider the ability to reach people with information by looking at the communications “channels” that are used. For prior information we could, for example, use written material which could be sent to homes and offices or made available on the internet, videos and websites on the internet, visitor centres, exhibitions or talks. The aim might be to engage, inform and gain trust wherever practical.
It is important to consider the range of scientific literacy of your target audience. Since we generally choose an area around a nuclear site it is likely to include a random set of people. Our role is to enhance their scientific knowledge to the level at which they can make reasoned decisions about their safety and the safety of their families and neighbours should an accident happen. It is probably best to assume little or no prior knowledge on the part of the general population and strive to present the required information and supporting basic concepts as simply as possible, providing a credible source of information and support in understanding the material.
The public may be more interested in the actual effects of radiation and how to avoid harm rather than the complexities of radioactivity and health physics. The form of the message may be important.
When we recommend to people in a particular area to shelter in place, we are saying to them “we believe that if you go indoors and shut the windows and doors then your ionising radiation dose over the remainder of this event will be reduced compared to your dose if you stayed outside for the duration, or tried to evacuate, and that this improves your long-term health chances by an amount that makes it worthwhile to stop what you are doing outside and go indoors”.
You may also have the opportunity to present information to a more expert audience such as the medical services in the area or to decision makers and managers in local businesses. They may or may not have more knowledge than the general public and may have different factors at play in their decision processes.
Current systems to warn the public are largely based on phone systems which send a message to registered land lines and broadcasts on conventional and social media. The land line telephone system may be expected to work well for occupied offices and homes but is not effective for people out in the open. Use of mobile phones gives a significant increase in capability in terms of ability to reach those who work in the open and are registered. The ability to message all mobile phones in an area is technically possible but, as of 2021, is being introduced painfully slowly in the UK. Radio and TV broadcasts and social media posts may reach those who listen to the radio/TV or who pay constant attention to their phone and have the right app or follow the right social media accounts but not others. There will always be gaps. The role of the planners is to identify who may not be served by current systems and consider if more should be done.
Recipient's decision
Some recent studies The Protective Action Decision Model: Theoretical, Methodological, and Practical Issues
in the USA looked at preparedness to survive severe weather events in areas where these are quite common.
They used the Protective Action Decision Model
(PADM) - The Protective Action Decision Model: Theoretical Modifications and Additional Evidence to frame their work.
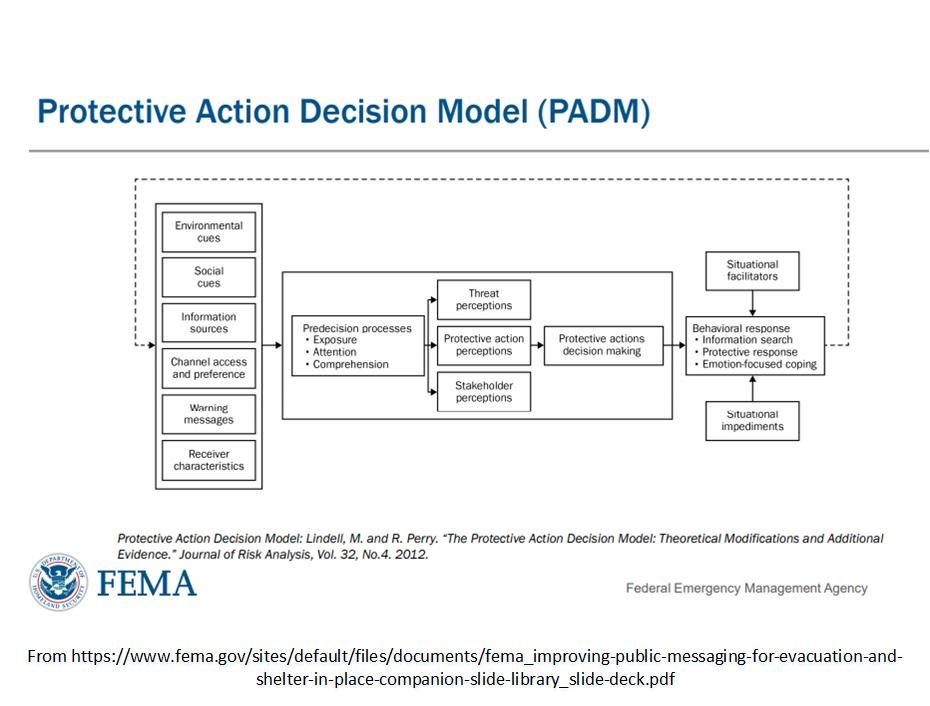
Many of these factors are things that we could, in principle at least, influence in a manner that increases the chances of a favourable outcome. Prior information can play on the person’s social cues, information sources, channel access and preferences, pre-decision processes and behavioural response leading to better decisions and improving the ability to take dose reducing protective actions with less stress to their mental health.
Following a comprehensive literature search the authors concluded that, despite public information programmes, some people are:
- unaware of any protective action for a given hazard;
- believe all recommended actions are ineffective; or
- believe all recommended actions require excessive resources.
These findings probably apply to the public’s preparations to cope with a radiation emergency in the UK to some extent.
The other lessons gleaned from the US study include:
- Do not talk to people about the probability that an event will happen; talk to them about the probability of that event’s consequences for them.
- Do not talk to people only about the probability of personal consequence; also talk to them about
- Protective actions being taken by authorities,
- Alternative protective actions they should consider,
- The characteristics of those protective actions, and
- Sources of assistance if this is needed to implement protective action.
A notable barrier to successful communication is the lack of understanding of radioactivity, radiation, radiation dose, the quantities of dose likely to be received by members of the public in a radiation emergency and the quantities of dose that are likely to damage health. The EU SHAMISEN Project (2017) recommended that we should “build a radiation protection culture between radiation protection experts, healthcare workers, professionals and the general public.” Where “radiation protection culture” is defined as “the understanding and know-how that is essential for a population to interpret monitoring results and, on that basis, be able to make informed decisions related to protective actions against existing or potential exposures to radioactivity”. This is laudable but well beyond the scope intended by current UK legislation which concentrates on informing the public and hopes that healthcare workers and professionals will rise to the challenge when called upon.
It is important to bear in mind the warning that “the system of radiation protection is based on science, but individual perception of risk and benefit is a legitimate and important factor, as behaviour is strongly driven by perception” (IRPA, 2020). The public perception of radioactivity significantly overestimates the risks. This was apparently in place before the second world war but became more firmly established by the debates on the potential impact of radioactive fallout following a nuclear bomb. It is found that “evaluations of risk are largely the result of emotions, rather than logic or facts. Although it is hard to recognize and accept that our perceptions may mislead us and curtail effective decision making, this is a well-established characteristic of humanity” (WNA, 2021). This limits the value of public information that is a stream of facts and well-meaning advice that fails to address the perception issue.
Perceived risk of radiation
See for example Slovic - It was shown that when asked to order 30 diverse matters such as nuclear power, handguns, motor vehicles,
pesticides, firefighting, swimming, skiing, food colouring in terms of risk, the league of women voters and active college students put
nuclear power at the top of the list compared to “experts” (presumably with access to statistics) who put it 20th.
This exaggerated fear of radiation, coupled with lack of trust of advice from the authorities, probably played a major role in the mass voluntary evacuation from around the Three Mile Island plant during the 1979 accident.
The perceived safety of stable iodine and the media – a warning
The media coverage of the relative risks and benefits of taking the AstraZeneca Covid-19 vaccine may give a warning to the nuclear industry about the ease with which populations can be encouraged to take an unfamiliar medicine and feel comfortable about their decision. Some European countries suspended their use of AstraZeneca in March 2021 on reports of a handful of cases where the blood clots had proven fatal, prompting national and international health authorities to investigate the reports. This resulted in increased “vaccine hesitancy” around the world and considerable social and mainstream media coverage.
Stable iodine must be taken within a few hours of exposure to radioiodine to be effective so the media dynamics will be quite different to the vaccine issue which developed over months. However, there may need to be some media management of the issue. It is quite likely that some of the people advised to take stable iodine in response to a nuclear emergency will seek information from the internet, from friends and from influencers they trust. The authorities must remain on top of any anti-iodine media surge.
A survey around a Japanese nuclear power plant restarted after the Fukushima event involved the sending of a questionnaire to 400 households and receiving 247 responses from within and beyond the PAZ. They found that 82 out of 94 (63%) guardians of children living in the PAZ were aware of the role of stable iodine in protecting child thyroids in a nuclear accident. Of these, 52 had taken possession of pre-distributed tablets. Reasons put forward for not collecting tablets included concerns about the potential side effects (40%) and distrust of the effectiveness (24%). This is despite significant effort to promulgate the value of stable iodine, including annual meetings and a brochure.
The perceptions of the public are not easily changed by simply presenting scientific facts and information. The Covid pandemic has shown how difficult it is to formulate, promulgate and justify advice to the public against the background of modern broadcast and social media. Experience has shown that the airwaves are suddenly full of opinion, expert and otherwise, that seeks to be heard, often expressing doubt that the official advice is correct or giving different interpretations as to what it means. Sooner or later a senior person appears on television and is challenged that the advice is wrong, arbitrary, too late and not understood. This is obviously unhelpful when you are trying to influence the population to behave in the manner that you estimate reduces their radiation dose by a useful amount.
Expert opinion v popular opinion
This daft post had a wide reach and influence. It was even discussed by the Prime Minister and Chief Medical Officer in a TV briefing.
Much of what is published prior to the event or broadcast on the day may not be understood or may not be actionable especially by people with barriers related to literacy, language, culture, or disability.
Despite this the UK government view, expressed on a slightly dated website HMG, Cabinet Office, 2018), is that “The government believes a well-informed public is better able to respond to an emergency and to minimise the impact of the emergency on the community. By informing the public as best they can, all organisations will build their trust. Part of this is also avoiding alarming the public unnecessarily. Meanwhile the National Steering Committee on Warning & Informing the Public (HMG, NSCWIP, 2013) seems to have faded away.
There are similarities with chemical incidents. The US Federal Emergency Management Agency (FEMA, 2021) tell us that “for a chemical incident, effective public communications involve the transmission of, via readily available channels, potentially lifesaving information to the population at risk of exposure in a manner that they can understand such that they will choose actions or behaviours that are protective of human and environmental health”.
In the UK, the Civil Contingencies Act requires Category 1 responders to “put in place arrangements to make information available to the public about civil protection matters and maintain arrangements to warn, inform and advise the public in the event of an emergency” and REPPIR-19 places responsibilities for warning and informing regarding radiation accidents onto the local authority.
By placing the warning and informing duty on many Category 1 responders the government is possibly reducing the chances of a truly capable system, designed and financed at national level. The US, by contrast, have the centrally funded Integrated Public Alert and Warning System (IPAWS) (FEMA, 2021b) which uses multiple pathways to reach as wide a range of people as practical. It is reported that there are more than 1,500 federal, state, local, tribal and territorial alerting authorities that use IPAWS.
The ability to act
No idea what to write here